






Will my rotator cuff heal? (or will the pain at least go away?)
- Jan 6, 2018
- 6 min read
This is one of the most common questions that I'm asked by patients with shoulder pain and a diagnosis of a rotator cuff tear. The answer, unfortunately, is not as straightforward as one may think. In addition, there is a tremendous amount of mis-information out there - some of it spread by other orthopedic surgeons! I'll try to sift through what we know (and what we don't know) about rotator cuff tears. I love this topic (and fixing rotator cuff tears) so this may turn into more than one post!

The rotator cuff is a group of four tendons (subscapularis, supraspinatus, infraspinatus, and teres minor) that surround the shoulder joint. They are responsible for range of motion, strength, and keeping the shoulder joint in the socket. Another muscle, the biceps, has a tendon that is intimately associated with these muscles, and is oftentimes involved in injuries to the rotator cuff.
Symptoms of a rotator cuff tear

The most common symptoms of a rotator cuff tear are pain and weakness. The pain from a rotator cuff tear is usually felt over the outside of the shoulder. It is typically worse with overhead activity. Night pain, even severe enough to wake you from sleep, is common with rotator cuff tears. Weakness is typically felt with the arm away from the body, with motion of the shoulder. Measurable weakness can be a later sign of rotator cuff tears, and typically indicates a relatively large tear.
Types of Rotator Cuff Tears
There are two main types of rotator cuff tears - acute and chronic tears. Acute rotator cuff tears are the result of an injury to the shoulder that dramatically increases shoulder pain. This can be minor trauma (a fall, or bumping into something) or major trauma (a car accident, etc). Symptoms will be the same as above. I recommend that patients with an acute rotator cuff tear get an MRI to look at the size of the tear. In some cases, these tears are very large and require semi-urgent surgery. There is some data that these should be fixed within about 6 weeks to 3 months. There are no rotator cuff tears that are "emergency" procedures...but we do like to work on these sooner rather than later. If the tear is left for too long (months or years), they can eventually heal in a bad position, or be unfixable (potentially needing a superior capsular reconstruction!).
Disclaimer: This is one area in which some surgeons are overly aggressive (we all like to operate on rotator cuff tears!). Even with acute rotator cuff tears, many tears are small, or partial. These may be treated without surgery, depending on your age and other factors. Be thoughtful and inquisitive if you are being told you need rotator cuff surgery. If you want me to review your MRI - I'm happy to. Contact information is above, or email (jonbarlowmd@gmail.com).
Chronic rotator cuff tears are tears that arise slowly over time, or without any injury. Symptoms are the same as above - pain in the shoulder, pain at night, and weakness with activity. These injuries, however, are happening slowly. Whereas acute rotator cuff tears require some urgency, there is little urgency to these issues. A careful, thoughtful approach to treatment can spare you unnecessary and even harmful surgery. Let's break things down further.
Partial and full thickness tear
This terminology is confusing, not only for patients, but for medical students, residents, and surgeons. There are a number of different ways that a rotator cuff tear can be described. The most common terminology is Partial vs Full thickness tearing. Full thinkness tearing is often called Complete tearing. As bad as "complete" sounds, it is oftentimes not as bad as you may think. Hint: it is never a complete tear of your entire rotator cuff....even with "massive tears" there is still a substantial portion of your rotator cuff that is intact.
A partial tear refers to any abnormality in the tendon, typically where it inserts to bone. This may be a bit of fluid in the attachment to the bone, a strain, or something more significant. In spite of our efforts to describe these in detail, we (surgeons and radiologists) cannot accurately describe much more than whether the tendon is attached or not. If it is attached and abnormal, it's a partial tear....if it is detached and there is a gap between the tendon and the bone, it's a full tear. This distinction is easy - you try:

Full or partial tear? Can you see the humerus, the large black shape in the middle? Follow the muscle on top, and see if you can follow it all the way to the bone. In this case, you can. The tendon is attached. There is some fluid in the tendon (a partial tear), but overall, the tendon is intact.

See, not that hard (I shouldn't give you all of our secrets). Now, let's look at a full thickness tear.

Can you see the tear? This is the opposite shoulder, but start again from the muscle, and follow the tendon. You will see that it doesn't attach to the bone. There is a gap between the tendon and the bone. This is a full thickness tear!

Now that you know that the tendon has torn off the bone (full thickness, or complete), we have to decide how large it is. This means assessing how much of the tendon has torn off the bone, and how much is still attached.

It is extremely uncommon to tear "the whole rotator cuff" off. Typically, complete tears begin in the supraspinatus (the top muscle). They enlarge and involve the other tendons as time goes by. Therefore, even in the setting of a "complete" or full thickness tear, the size is also important.
But the surgeon said I have a tear, that must need to be fixed!
Rotator cuff tears, like grey hair and wrinkles, are a normal part of aging. We have excellent studies that demonstrate this. With time, the rate of rotator cuff tears slowly climbs. The vast majority of patients, even with rotator cuff tears, have NO symptoms at all. Here's the data:
J Bone Joint Surg Am. 1995 Jan;77(1):10-5.
Abnormal findings on magnetic resonance images of asymptomatic shoulders.
Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB.
Findings on MRI of people with shoulders with NO SYMPTOMS:
40-60 year olds: 4% full thickness tear, 24% partial thickness tear
60 years old+: 28% full thickness, 26% partial thickness (54% had some tearing!)
J Shoulder Elbow Surg. 2014 Dec;23(12):1913-1921.
A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age.
Teunis T, Lubberts B, Reilly BT, Ring D.
Rotator cuff tears in patients with NO SYMPTOMS:
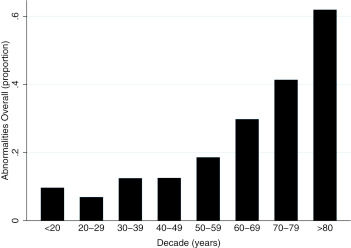
As you can see, like death and taxes, rotator cuff tears are inevitable. This shouldn't be disheartening though. Importantly, the patients in these studies had NO symptoms. That means that there are a large number of patients with partial or full thickness tears without any symptoms - encouraging news.
So what next?
There is compelling evidence that nonsurgical management (physical therapy) is effective for rotator cuff tears. If you have a partial thickness tear (acute or chronic) or a full thickness tear (chronic), this is where to start. The most well done studies on the topic indicate that up to 75% of patients with painful, full thickness rotator cuff tears will go on to have normal shoulders with physical therapy.

These results are remarkable. 75% odds are excellent. This group (which I have had the pleasure of being a part of) has done a number of studies to break this down.
They found:
Home exercises can be nearly as effective as ongoing formal therapy sessions (initial startup and teaching are important)
Activity level and demand on the shoulder don't matter
Size of the tear doesn't matter
The most important factor in recovery is whether or not patients thought therapy will work (the power of positive thought!)
Most patients, if they were going to improve, did so within about 6 weeks (certainly by 3 months)
Successful results are still present at 5 years from the start of therapy
The rotator cuff doesn't heal, it just becomes pain free!
Alright, I did the exercises for 6 weeks, my shoulder still hurts!
While many patients get better from physical therapy, some don't! This is where surgery is very effective. For patients with pain after therapy (home or formal), and full thickness tears, surgery is very effective. In these cases, I advocate an arthroscopic rotator cuff tear, using a "double-row" technique. I have operated on hundreds of patients for this reason, and the typical result is a pain-free, strong shoulder. While I do not advocate being overly aggressive with rotator cuff tears - surgical repair of rotator cuff tears remains a very cost effective, pain-relieving operation that can help patients return to full function.

Rotator cuff tears are a common finding in patients with or without shoulder pain. A thoughtful, conservative approach to evaluation and management of these tears is critical. Acute rotator cuff tears warrant an MRI and early surgical management. 6 weeks of PT (home or formal) is recommended for chronic rotator cuff tears. Arthroscopic fixation of full thickness tears that fail PT provides substantial pain relief and improved function.
Send me your questions or thoughts about rotator cuff tears - yours, or your patients (for providers)...I love thinking and talking about this common, but evolving problem.
Jon Barlow, MD
I read the post about whether a rotator cuff will heal and the pain might ease, and it really helped explain why some shoulder injuries take so long to feel better and what to expect from rest or treatment. When I was finishing a big paper in college I used Manuscript editing service late at night because my draft was confusing and needed to be clear before I shared it. That made me see how patience and careful work make a big difference.